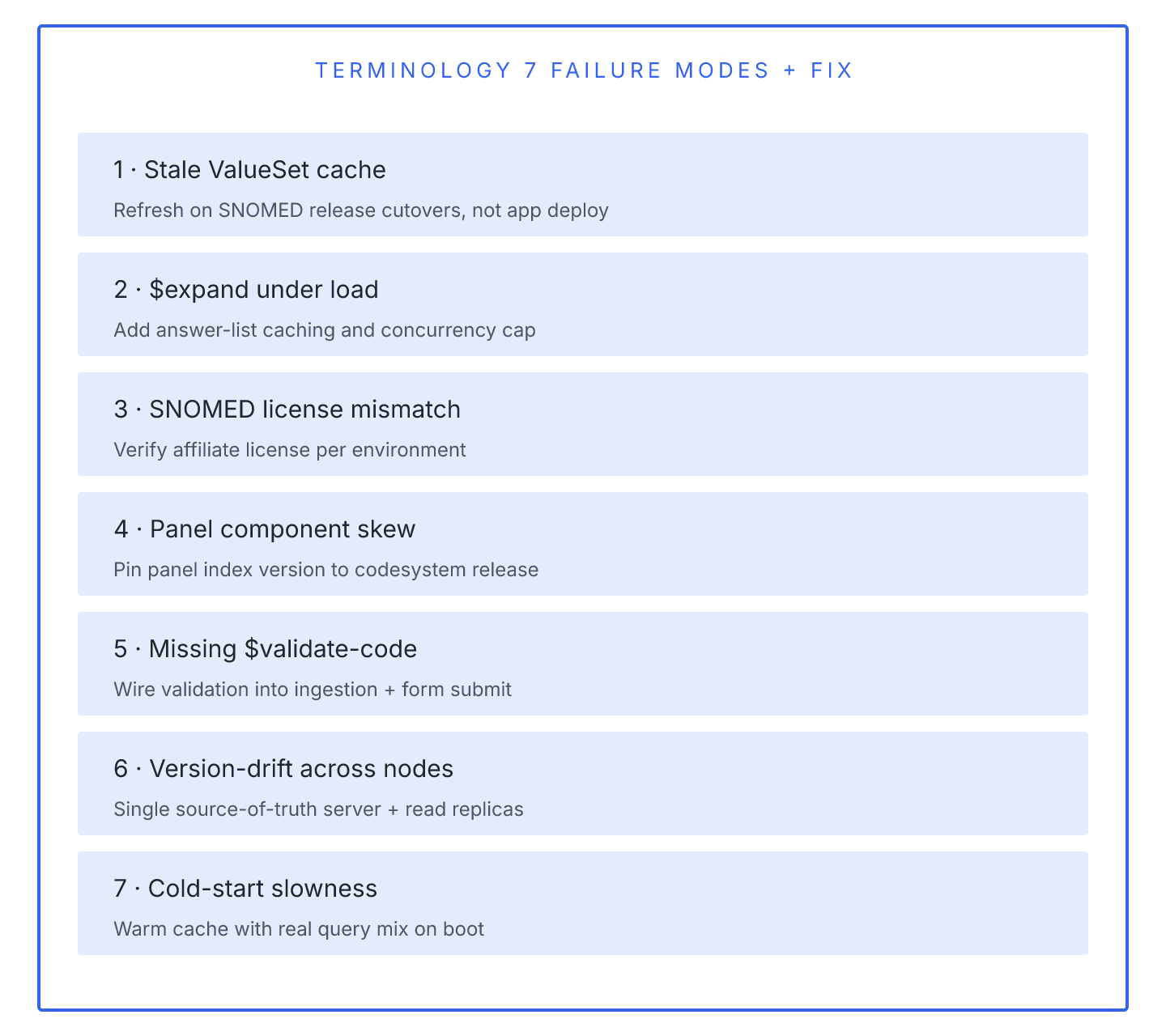
Wiring a FHIR terminology server into an existing EHR stack looks straightforward until the first $validate call returns a code that shouldn't have been accepted. The seven failure modes below cover almost every terminology integration incident we've seen in ambulatory and hospital deployments.
1. Missing code system version pinning. ValueSet definitions in US Core reference specific SNOMED CT and LOINC versions. Terminology servers that expand against latest-loaded codes drift from the profile bindings and start accepting codes retired in the pinned version. Fix: pin system|version explicitly in ValueSet.compose.include.
2. $expand timeouts on large ValueSets. SNOMED-based ValueSets can expand into tens of thousands of concepts. Servers that expand synchronously time out on 30-second HTTP defaults. Ontoserver offers paginated expansion; HAPI's terminology module supports offset+count parameters. Cache expansions for stable ValueSets rather than expanding per-request.
3. Silent code substitution. Some servers auto-map unknown codes to nearest siblings during $translate, without flagging the substitution. Downstream analytics then miscount conditions. Check the server's $translate conformance against the terminology module spec before trusting mapping output.
4. Concurrent $expand deadlocks. HAPI's JPA terminology tables use row-level locking that can deadlock under concurrent expand requests. Fix: separate read replica for terminology, or move to a dedicated terminology server.
5. RxNorm licensing gaps. RxNorm requires UMLS licensing and monthly updates. Terminology servers running against a snapshot from six months ago quietly emit outdated code labels. Automate the update pipeline.
6. Cross-server terminology mismatches. Multi-server deployments where each has its own terminology cache introduce drift. Centralize terminology at one authoritative server, use FHIR terminology proxy calls from others.
7. $lookup performance at scale. $lookup on individual codes is fast; batching lookups for hundreds of codes per validate call is not. Implement client-side caching of static code metadata.
Terminology server integration is a solved problem in 2026 provided your team treats it as its own subsystem with its own SLA. The mistake most teams make is bolting terminology onto the EHR as an afterthought.